Hip Pain That Won't Go Away: What We Look For Instead

That deep ache in your hip shows up after sitting through a long meeting. Squats feel pinchy. Walking uphill triggers discomfort that wasn't there two weeks ago.
You've stretched your hip flexors, foam rolled, done the clamshells your physiotherapist recommended. It helps temporarily, then returns the moment you resume normal training.
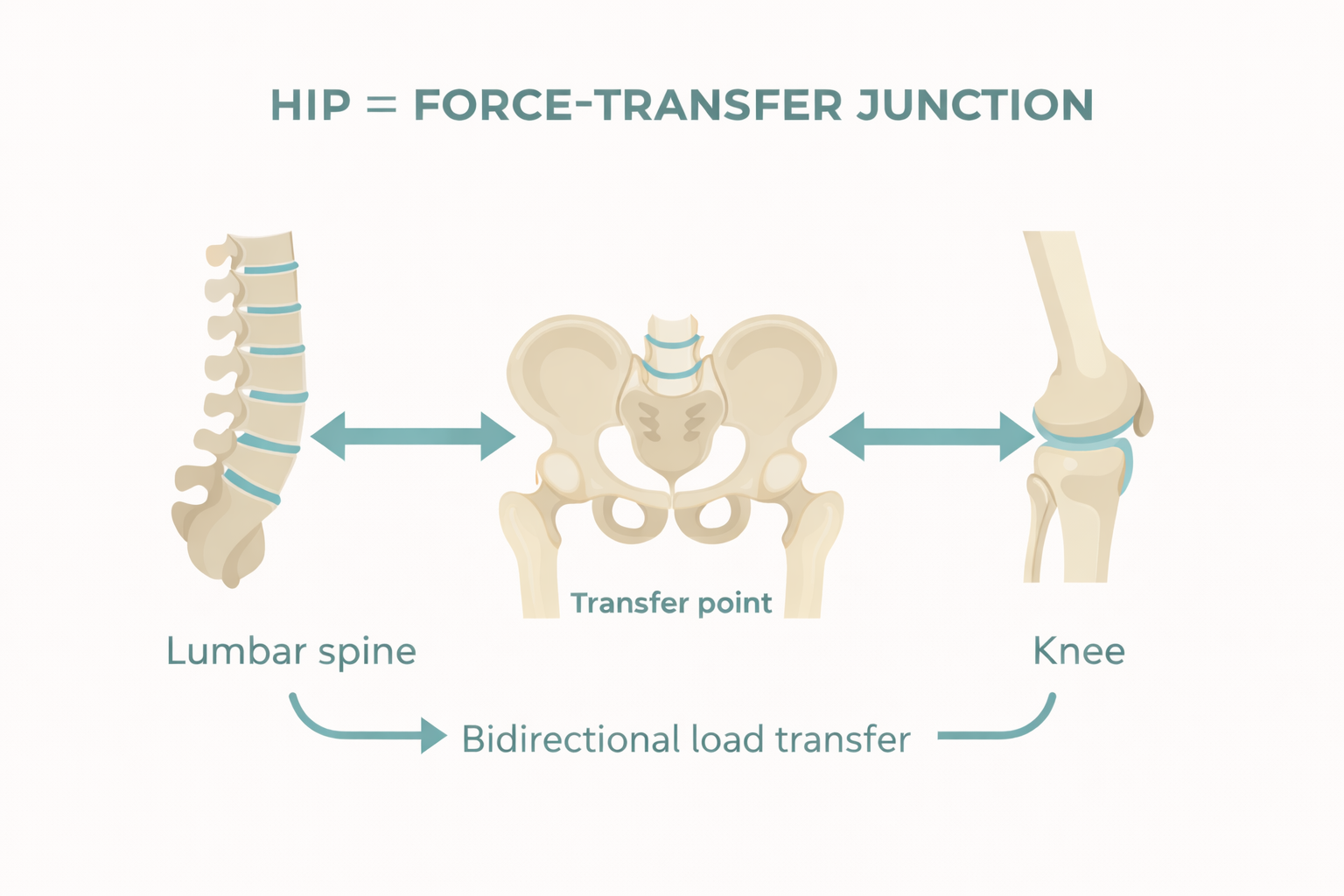
Here's what everyone misses: your hip is the middleman, not the culprit. It sits between your spine and knee, transferring force bidirectionally. When either end fails to contribute, your hip absorbs the fallout.
(Evidence background: kinetic chain load transfer concepts and the lumbopelvic–hip complex as a central transfer point.)[1]
The Hip as Force-Transfer Crossroads
Your hip is a major force-transfer junction between spine and knee. When functioning properly, it controls movement and distributes load efficiently.
When it doesn't, stress redistributes:
Upward into your lower back
Downward into your knee
Or concentrates locally at the hip itself
Recognize these?
"Sitting too long aggravates my hip"
"Squats cause anterior hip pinching"
"My hip pain started after my back issues began"
This isn't isolated hip damage. It's compensation for failures elsewhere.
Four Systems That Dump Load onto Your Hip
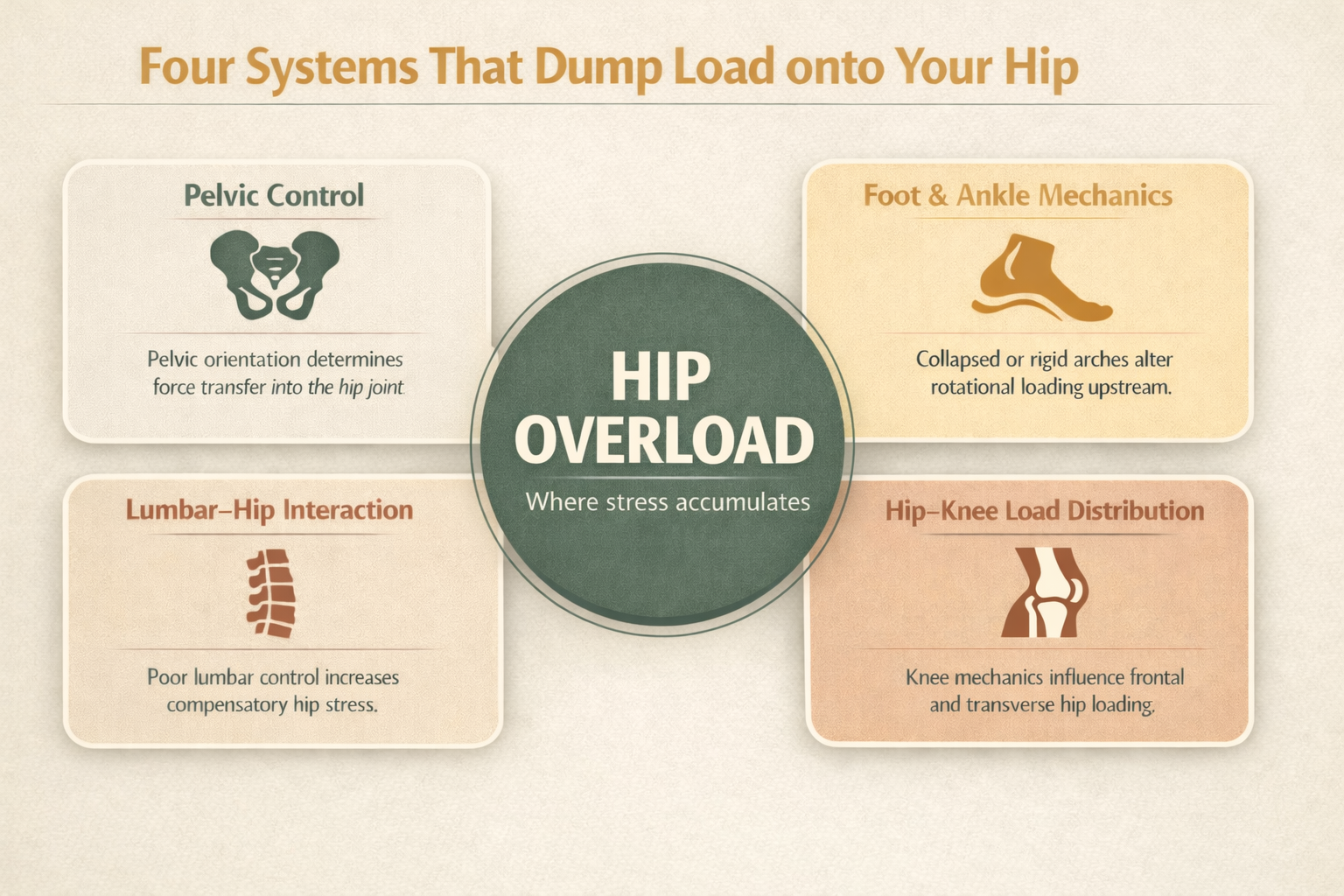
Your hip's load tolerance depends on pelvic positioning, force entry through your feet, spinal load transfer, and movement sharing with your knee.
When these systems fail, your hip becomes the default shock absorber:
Pelvic control dysfunction: When your pelvis lacks stability or proper positioning, your hip loses efficient load sharing. This appears as discomfort during prolonged sitting, standing, or squat depth—especially anterior hip pinching.
Foot mechanics breakdown: Collapsed or excessively rigid feet cause inefficient force transmission up the chain. Your hip manages stress it wasn't designed for, typically manifesting as lateral hip or glute tension.
Lumbar stiffness: When your lower back lacks mobility or control, your hip compensates by moving excessively—or stabilizing when it should move. This is particularly common when your pelvis and spine move as one locked unit.
Knee avoidance or dominance: When your knee avoids load, your hip picks up the slack. When your knee dominates, your hip compensates. The pain shows up at whichever joint is handling disproportionate stress.
Your hip isn't weak. It's overloaded.
Why Hip Pain Location Is Notoriously Vague
Hip pain is difficult to localize: deep in the joint, anterior hip, lateral glute, groin?
The hip's complex muscular and connective tissue attachments make pain location unreliable. Where you feel pain reflects how force enters or exits the hip—not which structure is damaged.
Location provides investigation clues, not diagnostic conclusions.
Our Toronto Hip Assessment: Tracking Load Through the System
We don't isolate your hip. We assess load transfer through your entire kinetic chain.[2]
Pelvic Position and Control
Does your pelvis provide a stable foundation for hip movement? Limited pelvic control means your hip:
Loses efficient load sharing
Stays in end ranges excessively
Stabilizes when it should move
Foot and Ankle Mechanics
Force enters through your feet. Collapsed or stiffened feet force your hip to manage inappropriate loads. This typically presents as lateral hip tension or pain exacerbated by prolonged walking.
Lumbar-Hip Interaction
Limited lumbar mobility forces hip compensation—either excessive movement or inappropriate stabilization. This pattern intensifies when your pelvis and spine function as one rigid segment.
Hip-Knee Load Distribution
Your hip and knee function as partners. When one dominates or avoids contribution, the other compensates. We assess load sharing patterns—not just pain location.
Movement Strategy Assessment
We evaluate walking, hinging, squatting, and weight-shifting patterns. These reveal why hip pain emerges only at specific volumes, intensities, or positions.
Why Hip-Focused Treatment Produces Temporary Results
Stretching, foam rolling, and isolated hip strengthening provide temporary relief. They reduce symptoms and improve short-term tolerance.
But they don't address how load transfers through your hip.[3]
The predictable cycle:
Temporary improvement
Gradual pain return
Progressive movement limitations
This is the most common pattern with chronic hip pain in Toronto.
Assessment Before Intervention
We assess before adding exercise or intensity. Our evaluation examines:
Pelvic position and control
Foot and lower limb mechanics
Lumbar-hip interaction
Load transfer patterns
This identifies where compensation occurs and why.
Explore our 90-minute assessment.
Corrective Exercise: Restoring Load Transfer
Corrective exercise for hip pain isn't about isolated muscle strengthening. It's about restoring efficient load transfer:
Improving pelvic control and positioning
Restoring hip-knee-foot coordination
Teaching efficient force distribution
Rebuilding strength through improved patterns
Learn about our training methodology.
If Treatment Hasn't Resolved Your Hip Pain
Persistent hip pain despite treatment, rest, and modification reveals:
Inefficient load transfer patterns
Hip compensation for spine, knee, or foot dysfunction
Unidentified underlying patterns
Your hip isn't damaged. The system needs assessment.
Start With System Assessment
Recurring hip pain in Toronto deserves clear answers, not generic advice.
We'll evaluate pelvic control, foot mechanics, and load-transfer patterns to identify what's driving your hip pain—and determine if our corrective approach fits your situation.
Book your free consultation here.
Sources
Role of kinetic chain in sports performance and injury risk: a narrative review (open access): https://pmc.ncbi.nlm.nih.gov/articles/PMC10893580/
Current concepts: the hip, core and kinetic chain in the overhead athlete (PubMed): https://pubmed.ncbi.nlm.nih.gov/38007174/
The Influence of Stretching the Hip Flexor Muscles on Performance Parameters: systematic review + meta-analysis (open access): https://pmc.ncbi.nlm.nih.gov/articles/PMC7922112/