Why Your Shoulder Pain Keeps Coming Back
Reaching overhead to grab something from the top shelf shouldn't hurt. But there it is again—that sharp pinch in your shoulder.
You've backed off from pressing exercises. You've stretched. Maybe you saw a physiotherapist. The pain improves, then returns the moment you push intensity again.
Here's what most approaches miss: your shoulder isn't the problem. The platform it's moving from is.

The shoulder is the most mobile joint in your body. That mobility requires a stable, well-positioned foundation. When your rib cage, mid-back, and neck fail to provide that foundation, your shoulder compensates—and eventually breaks down.
Why Your Shoulder Keeps Breaking Down
Chronic shoulder pain doesn't originate at the shoulder. The shoulder's extreme mobility demands precise positioning from the rib cage, thoracic spine, and neck.
When those systems fail, your shoulder manages stability it was never designed to handle alone.
Recognize these?
"Overhead movements hurt"
"Pressing feels fine until suddenly it doesn't"
"My shoulder improved with treatment, then the pain returned"
The pain is real. But it's the result of poor positioning and inadequate trunk support—not isolated shoulder damage.
Four Foundation Problems That Cause Shoulder Pain
Your shoulder's ability to move freely and tolerate load depends entirely on what's underneath it:
Rib cage + breathing mechanics: A chronically flared or collapsed rib cage usually comes with shallow, chest-dominant breathing. That combination locks the trunk into poor positions, reduces stability during arm movement, and forces the neck and shoulder muscles to become stabilizers. Over time this can inhibit key scapular muscles such as the serratus anterior, degrading scapular upward rotation and shoulder mechanics.[1]
Thoracic spine stiffness (kyphotic posture): An excessive thoracic curve and rounded-shoulder posture reduces overhead capacity. It also shifts work away from the trunk and scapula and into the front of the shoulder.

Neck and cervical dysfunction: Excess cervical tension alters scapular positioning and increases shoulder muscle tone. Most people with chronic shoulder pain also experience recurring upper trap tightness or neck stiffness.
Load transfer failure in pushing patterns: Many clients press by driving the shoulder forward instead of distributing load through the chest and trunk. The humerus loses centered control, the anterior deltoid takes over, and overhead pressing overloads the front of the shoulder.[2]
Your shoulder isn't weak. It's operating from a compromised platform.
Why Shoulder Pain Location Misleads
Shoulder pain feels specific: front deltoid, top of the shoulder, deep in the joint, radiating down the arm.
One example is the long head of the biceps tendon, which can drive pain felt at the front of the shoulder.
But the shoulder's complex muscular and connective tissue attachments make local symptoms unreliable. Pain in one spot doesn't identify the problem structure—it reflects how force transfers through your arm and trunk.
This is why treating the shoulder in isolation produces temporary relief but rarely lasting change.
Our Toronto Shoulder Assessment: Evaluating Position and Support
When clients present with chronic shoulder pain, we don't treat the shoulder. We assess how it's being positioned and supported during movement.
Rib Cage Position
Your rib cage provides the foundation for shoulder mechanics. Excessive flaring or collapsing eliminates the stable base your shoulder needs, causing:
Early fatigue during arm movements
Pinching sensations overhead
Poor load control through full ranges
Neck and Cervical Mechanics
Your neck and shoulder function as an integrated system. That connection is why it’s hard to have a persistent shoulder problem without the neck eventually getting involved—and why stubborn neck dysfunction often shows up as shoulder pain or shoulder control issues.
Cervical dysfunction:
Alters scapular positioning
Increases shoulder muscle tone
Restricts shoulder mobility
Clients with chronic shoulder pain almost always report concurrent neck stiffness or upper trap tension.[3]
Thoracic Mobility
Your mid-back enables efficient shoulder movement. Limited thoracic mobility forces compensatory shoulder movement—particularly during overhead and rotational tasks.
This compounds stress on local shoulder tissues over time.
Breathing Pattern Assessment
Breathing simultaneously affects rib position, spinal support, and shoulder mechanics. Dysfunctional patterns:
Lock your rib cage into compromised positions
Reduce trunk stability during arm movement
Force neck and shoulder muscles to compensate as stabilizers
This is the most commonly overlooked driver of chronic shoulder pain.
Load Transfer Patterns
How you introduce and control load determines shoulder stress. We evaluate:
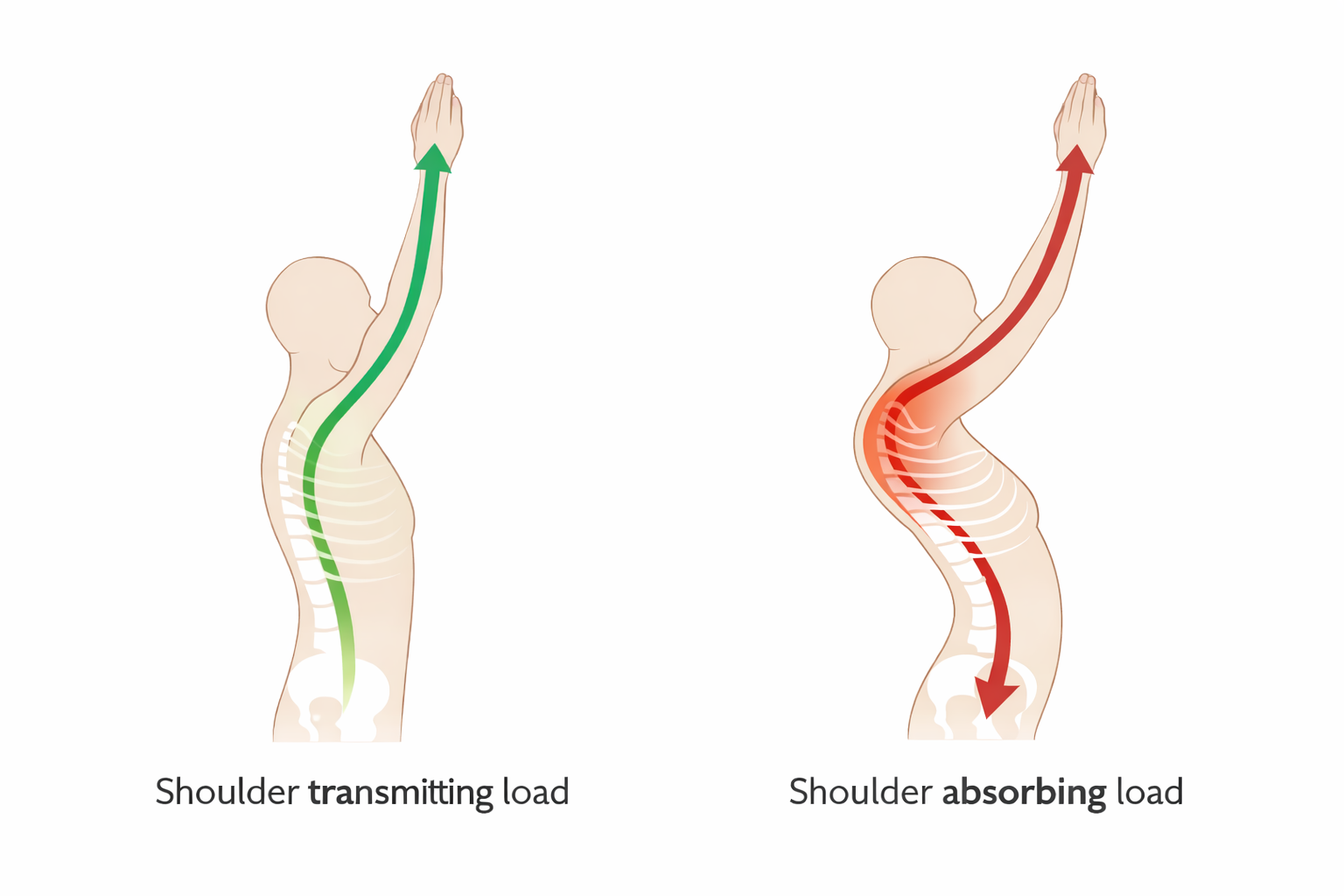
Force transfer from hand to trunk
Whether your shoulder absorbs or transmits load
How fatigue degrades movement strategy
These patterns explain why pain appears only at specific volumes or intensities.
Why Shoulder-Focused Treatment Fails
Rest, stretching, massage, and isolated shoulder exercises provide short-term relief. They calm irritation and improve tolerance temporarily.
But they don't address how your shoulder is positioned and loaded.
The predictable outcome:
Brief improvement
Gradual pain return
Progressive limitations with training or daily activities
This is the most common pattern we see with chronic shoulder pain in Toronto.
How Assessment Reveals the Real Problem
We start with assessment—before treatment, exercises, or assumptions. Rather than targeting the shoulder, we evaluate:
Rib cage and thoracic positioning
Cervical mechanics
Breathing patterns
Shoulder movement under controlled load
This identifies where compensation occurs and why—before we add strength, volume, or intensity.
Explore our assessment methodology.
Corrective Exercise: Rebuilding the Foundation
Corrective exercise for shoulder pain doesn't mean avoiding overhead work or protecting the joint indefinitely.
It means:
Restoring proper rib cage, thoracic, and cervical positioning
Teaching integrated shoulder-trunk movement
Progressively rebuilding strength without reinforcing compensation
This is why our approach differs from traditional shoulder rehab programs.
Learn about our training philosophy.
If Treatment Hasn't Resolved Your Shoulder Pain
Persistent shoulder pain—despite treatment, rest, or modification—reveals important information:
Your shoulder is compensating for poor positioning elsewhere
Load isn't distributing effectively through your trunk
The underlying pattern hasn't been identified
This doesn't mean your shoulder is damaged. It means the system needs assessment.
Start With Foundation Assessment
Recurring shoulder pain in Toronto deserves clear answers, not guesswork.
We'll evaluate rib cage position, thoracic mobility, cervical mechanics, and breathing patterns to determine what's driving your shoulder pain—and whether our corrective approach is right for you.