How to Describe Pain So You Can Fix It — Pain Literacy for office Workers

TL;DR
If you can describe where your pain is, what it feels like, when it shows up, what triggers it, and what relieves it, you’ll get to the right plan faster — and stop guessing.
This isn’t about being dramatic. It’s about being specific.
Who this is for
If you're a 40+ office worker who gets recurring back/hip/neck/shoulder flare-ups (often "randomly"), this is for you — but not limited to you.
A few things I hear often:
"I don't know… it just hurts."
"It's probably just arthritis."
"I'm getting older — this is my new normal."
Before we get into the checklist, three quick reframes worth having:
"This is just my age." Age-related changes are real. But most recurring pain patterns are driven by position, movement strategy, and load tolerance — not just years. Common doesn't mean inevitable.
"It's probably arthritis." Maybe. But most people treating "arthritis pain" are treating a label, not the driver. The pattern — where it is, what it feels like, what triggers it — tells us more than the word does.
"A 6 is a 6." Two people can both say 6/10 and have very different situations. One ramps up fast and lingers for days. The other warms up and settles quickly. Irritability, linger time, and what you can't do are usually more useful than the number.
The problem in all three cases is the same: vague thinking leads to vague decisions. When we can name the pattern, we can choose the right next step — and actually track whether we're improving.
The big idea: pain has a pattern (not just a number)
Pain isn’t just “good” or “bad.” It has:
Location (where)
Quality (what it feels like)
Behavior (when it shows up + what it does over 24 hours)
Context (what changed recently)
If we understand the pattern, we can make better calls about training, movement, recovery, and when to get medical help.
The Pain Language Checklist
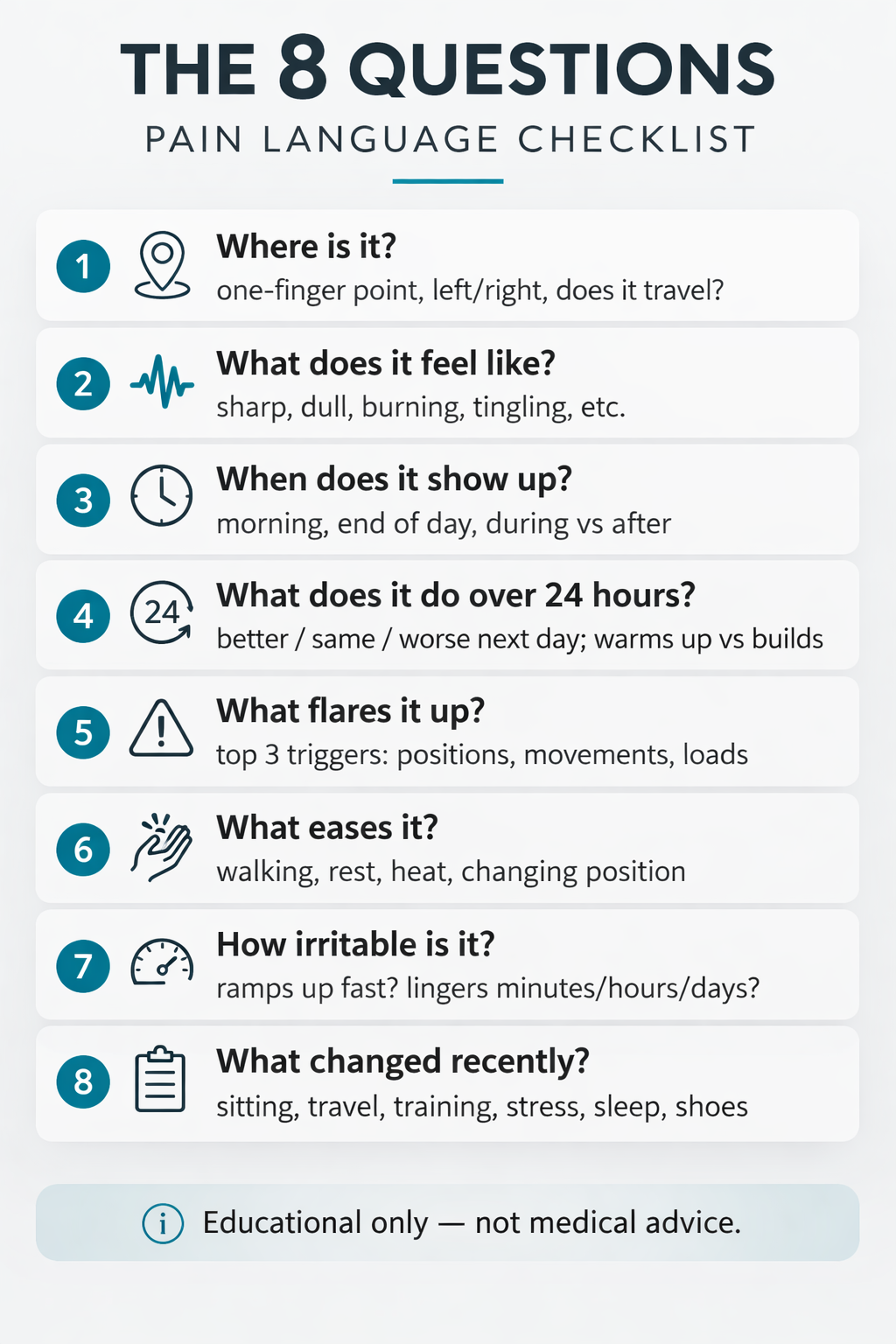
Quick rule: If you can’t point to it with one finger, describe the edges (top/bottom/inside/outside) and the position or movement that reproduces it.
1) Where is it?

Try to answer like you’re giving directions.
Can you point to it with one finger?
Is it front / back / side?
Is it left / right / both?
Is it above or below the joint? (Example: “2 inches below my knee on the inside.”)
Is it one spot, an area, or a trail?
Does it travel or radiate? (Where to where?)
Any tingling, numbness, or burning? If yes, where does the line/path run?
Why this matters: location and travel patterns can change the plan completely.
2) What does it feel like? (quality)
Pick the best matches. If you’re not sure, pick two.
These are clues, not diagnoses — we use them to choose safer modifications and decide next steps.
Color key (severity + what to do next):
Red: high severity / higher risk isgnal. Stop or modify now. If it doesn’t improve quickly with a simple change, get assessed (physio/doctor as appropriate).
Yellow: moderate severity / caution. May be training-load, recovery, or strategy related; adjust and monitor the 24-hour trend (sometimes it’s a sign it needs rest).
Green: low severity signal that’s generally OK to continue with — should be localized, controllable, and resolve predictably.
Sharp / stabbing — often a warning signal (modify/stop and reassess)
Dull / achy — often a load/tissue tolerance or joint irritation clue (context matters)
Burning — localized muscle burn during hard work (if it feels hot/electric or travels, treat it as a nerve-type clue)
Electrical / shock-like — often a nerve-related clue (especially if it travels)
Tingling / numbness — often nerve-related; depending on position/activity it can also reflect circulation restriction (track the exact area/path)
Catching / pinching — often a position/alignment or movement-strategy clue
Tight / crampy — often fatigue/guarding; sometimes hydration/electrolytes (e.g., potassium/magnesium) can be a factor
Stiff / blocked — often protective guarding or joint stiffness (context matters)
Throbbing / pulsing — often a higher-irritability/inflammation-type signal (context matters)
Weakness — often nerve-related (or a “shut down” signal when the system doesn’t trust the position)
Why this matters: the type of pain helps identify the likely driver — which changes the prescription.
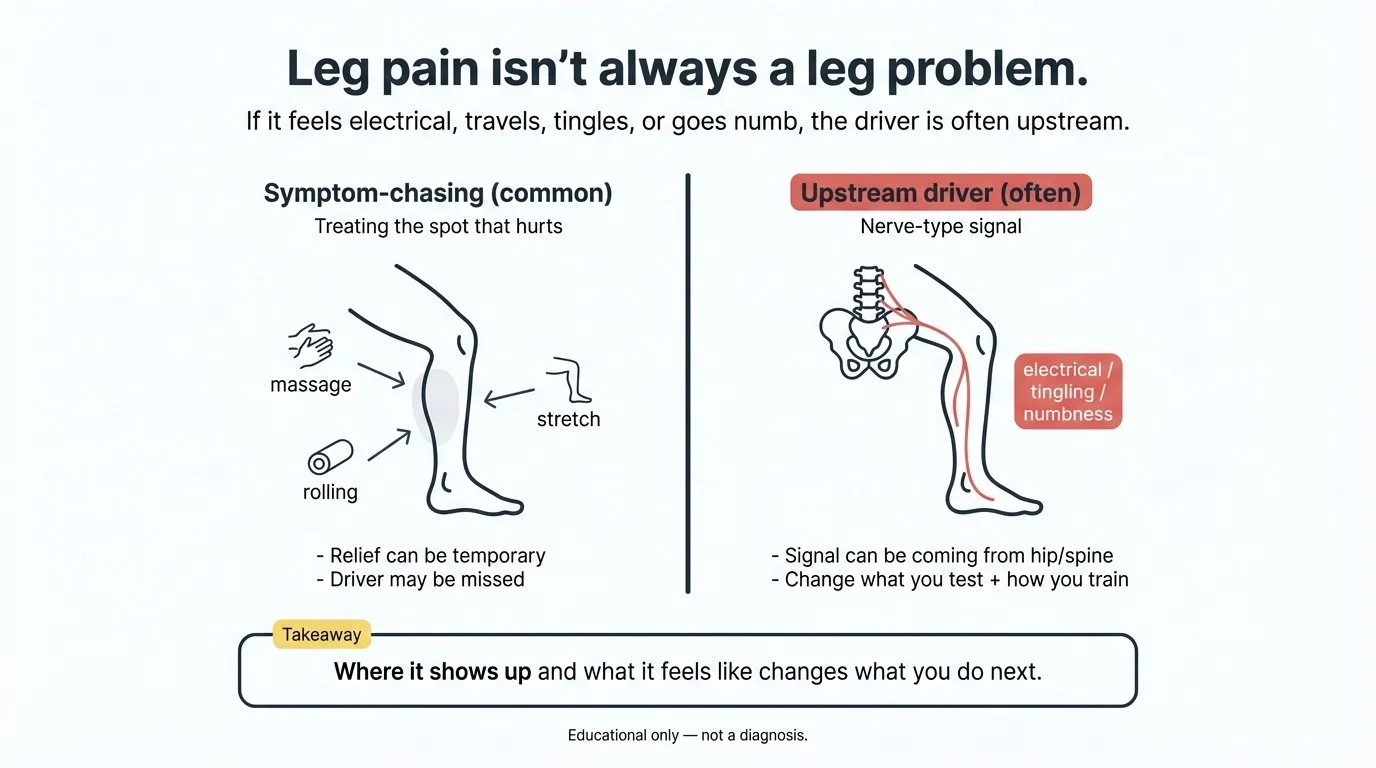
Example: if you say "my leg hurts," it's easy for people to chase the symptom (massage the leg, stretch the leg, roll the leg) and never get a lasting change. But if you tell me it feels electrical/shock-like (or it travels, tingles, or goes numb), there's a good chance the driver isn't in the leg tissue at all — it may be coming from the hip or spine — which completely changes what we test and how we train.
If radiating leg pain is part of your pattern, What's Actually Causing Your Sciatic Pain goes deeper on the two most common drivers and why distinguishing between them changes the plan.
3) When does it show up? (timing)
Morning vs end of day
First 5 minutes vs after 30 minutes
During activity vs after activity
Why this matters: timing often tells us whether you’re sensitive to certain positions, loads, or fatigue.
4) What does it do over 24 hours? (high signal)
Two of the most useful questions:
How does it feel the next day? (better / same / worse)
Does it “warm up” as you move, or does it build as you go?
Why this matters: the 24-hour pattern is often more important than what you feel in the moment.
5) What flares it up? (your top 3 triggers)
List your top 3.
Positions: sitting, bending, standing, driving, sleeping
Movements: stairs, squats, reaching, turning
Loads: carrying groceries, training, shoveling
Then add precision:
Worse with speed, or worse with depth/range?
Worse with repeated reps, or just one rep?
Worse holding a position, or moving in/out of it?
Why this matters: this is how we find the “driver.”
6) What eases it?
What changes the signal?
Walking?
Rest?
Heat?
Changing position?
Gentle movement?
Specific stretches?
Why this matters: relief patterns are clues, not just comfort.
7) Intensity and irritability (not just 0–10)
The number is helpful, but these are often more helpful:
How quickly does it ramp up?
How long does it linger after you stop? (minutes / hours / days)
What does it stop you from doing? (sleep, stairs, training, sitting, picking up kids)
Two important “non-negotiables” (safety rules):
Any nerve-type pain (electrical/shock-like, tingling, numbness, radiating lines, true weakness) is a red signal even at 1/10: stop or adjust immediately. Nerves recover slowly, and you don’t want to keep feeding an irritated nerve.
Sharp/stabby pain at any level is also a red signal: stop/adjust immediately. If it doesn’t settle with a simple modification, get assessed (physio/doctor as appropriate).
My coaching rules for training discomfort:
If the sensation is clearly muscular and localized, I generally don’t want you “training into it” if it’s more than about 3–4/10. Past this range you not only increase injury risk, you often start compensating — which can negate the benefits of the exercise altogether. We’ll modify the exercise so you can train the muscle without aggravating the signal.
If we can’t modify an exercise to get symptoms to 0/10, then we stop that exercise — even with coaching and supervision. At that point, either there’s an injury that needs to be respected, or the pattern needs to be reprogrammed at a much lighter load / simpler variation first.
Why this matters: irritability tells us how careful we need to be — and how to progress safely.
8) Baseline context (what changed)
Two simple questions:
What changed recently? (new activity, more sitting, travel, new shoes, new training plan, stress, poor sleep)
Have you had this exact thing before? (yes/no)
Why this matters: pain often shows up when inputs change faster than your body’s current tolerance.
Training discomfort vs warning signals (simple rules for training)
A lot of people either avoid all discomfort (and never build tolerance), or they push through warning signals (and flare up).
This section is just a practical summary — the details live in the checklist above.
Here’s a simple way to think about it:
Lower-severity training discomfort usually looks like:
Effort, muscular burn, or fatigue
A clear connection to the working muscle
Resolves predictably within 24–48 hours
Doesn’t change your mechanics (you don’t have to limp, twist, or brace weirdly)
Higher-severity warning signals often look like:
Sharp, catching, pinching pain
Nerve-y sensations: burning, tingling, numbness, radiating lines
Pain that escalates rep-to-rep or set-to-set
Pain that lingers or worsens over the next 24 hours
Pain that makes you move differently (compensation)
What to do if you hit warning signals
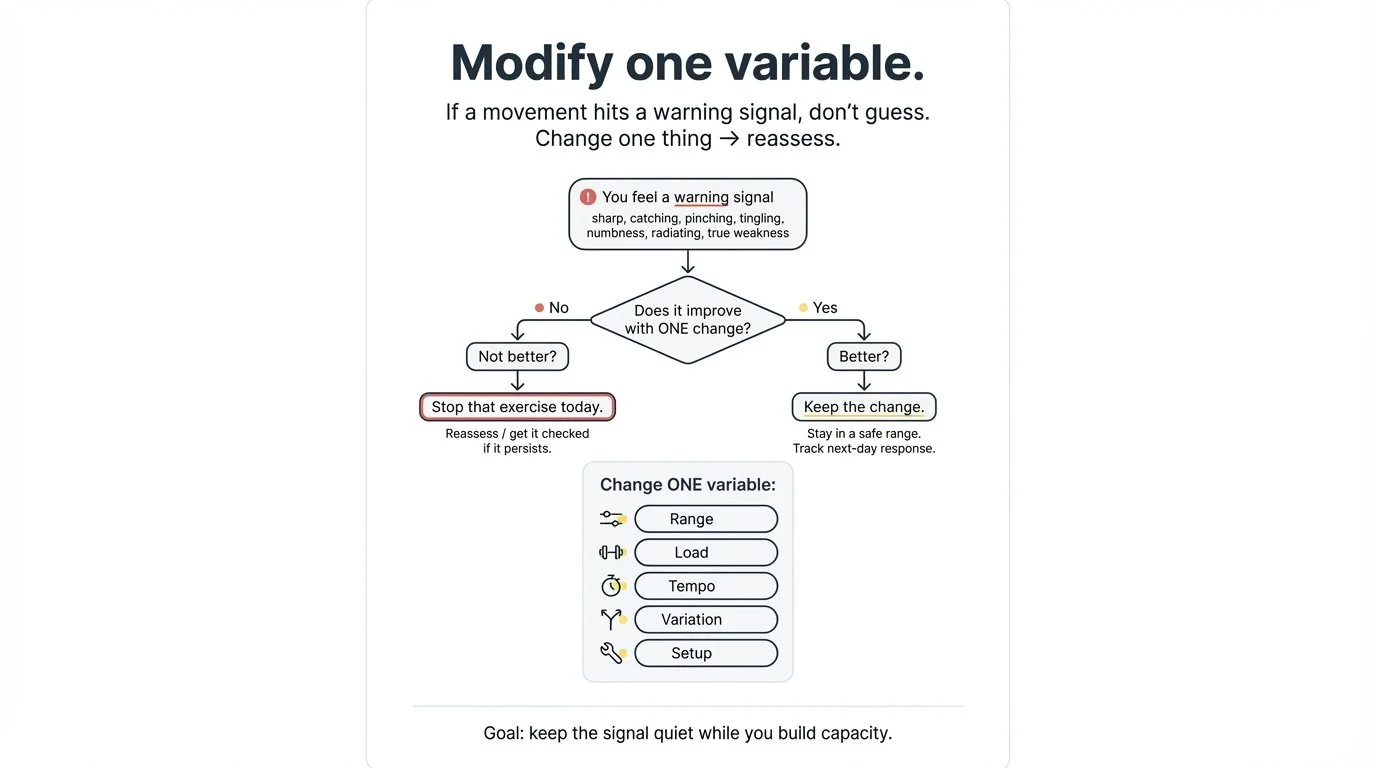
Don’t guess. Run a quick “modify one variable” test:
Reduce range
Reduce load
Slow tempo
Change the variation
Change your setup (stance, grip, breathing, positioning)
If the signal improves, you found a better path.
If it doesn’t improve, that’s useful information too: stop and reassess.
Red flags (when to seek medical help)
If you have any of the following, seek medical attention:
New numbness or weakness
Loss of bowel or bladder control
Unexplained fever
Severe, unrelenting night pain
Recent major trauma
When to get it checked (even if it’s not an emergency)
If you’re training without supervision, don’t let symptoms linger and become your new baseline.
Consider getting assessed by a qualified clinician (doctor/physio as appropriate) if:
Pain persists more than a few days without a clear trend of improvement
Pain is getting progressively worse week-to-week
You have lingering or recurring nerve-type symptoms (electrical/shock-like pain, tingling, numbness, radiating lines, or true weakness)
If you're in Etobicoke or the west end of Toronto, here's what our assessment process looks like.
About imaging (practical note)
Imaging isn’t always required, but if you’re concerned about nerve-type symptoms or something isn’t improving, it’s reasonable to ask your clinician whether imaging is appropriate and what the plan is if symptoms don’t settle.
If you’re told imaging isn’t indicated, you can ask for clarity on:
What they think is most likely going on
What signs would change the plan (and prompt imaging or referral)
That your symptoms and your request were documented in your chart
The goal isn’t to “fight the system” — it’s to make sure your symptoms are taken seriously and you have a clear, documented plan.
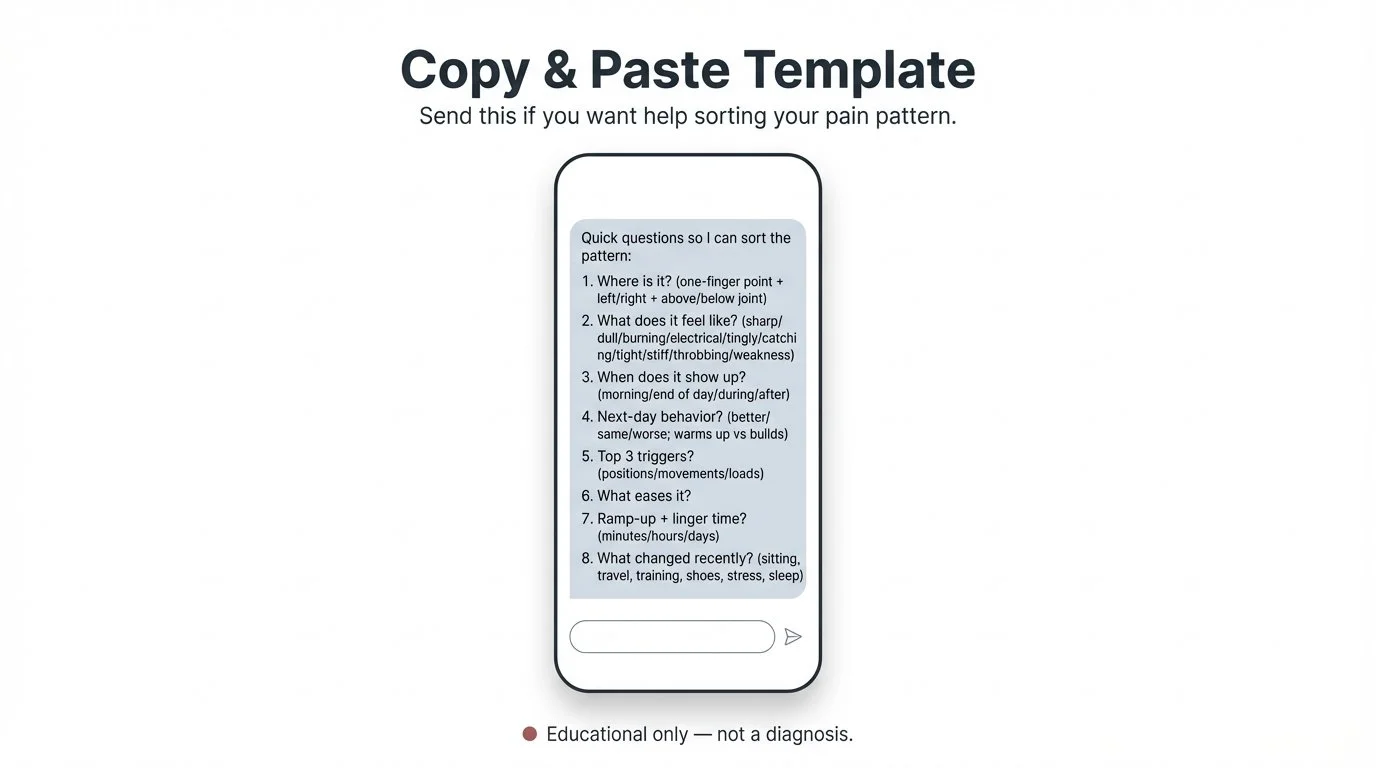
Copy/paste DM template
If you want help decoding your pain pattern, copy/paste this and send it:
Where is it? (one-finger point + left/right + above/below joint)
What does it feel like? (sharp/dull/burning/electrical/tingly/catching/tight/stiff/throbbing/weakness)
When does it show up? (morning/end of day/during/after)
Next-day behavior? (better/same/worse; warms up vs builds)
Top 3 triggers? (positions/movements/loads)
What eases it?
Ramp-up + linger time? (minutes/hours/days)
What changed recently? (sitting, travel, training, shoes, stress, sleep)
If you want a clear plan that helps you train without flare-ups, book an assessment — we'll map your pattern, find the driver, and build the next steps from there.
For more on what that looks like for adults managing recurring back or hip pain, see our blog post on how the location of your pain is rarely the source of the problem.
FAQ
-
Start with where it is (one-finger point, left/right, above/below the joint), what it feels like (sharp/dull/electrical/burning), when it shows up (morning, after sitting, during activity), and what makes it better or worse. The more specific you are, the faster you get to the right plan.
-
Pain that moves — especially electrical, tingling, or numb sensations — often suggests a nerve is involved somewhere along its path. The source may not be where the pain shows up. This distinction changes what you do next, which is why it matters.
-
Muscle soreness is usually localized, dull or achy, predictable, and settles within 24–48 hours. Warning signals tend to be sharp, electrical, or radiating — they may escalate rep-to-rep and often linger well past the workout. When in doubt, treat it as a warning signal and adjust.
-
It depends on the type. Effort, muscular burn, and mild local achiness are usually fine to train through with appropriate modifications. Sharp, stabbing, electrical, or radiating pain are red signals — stop the exercise, try a modification, and if the signal doesn't settle, don't push through it.
-
Irritability describes how easily the pain ramps up and how long it lingers after provocation. High irritability means it flares quickly and settles slowly. This is often more useful than a 0–10 number alone because it tells you how carefully to load and progress.
-
If pain persists more than a few days without a clear trend of improvement, gets progressively worse week to week, or involves nerve-type symptoms (electrical/shock-like, tingling, numbness, or weakness), it's worth getting assessed. Don't let a recurring pattern become your new baseline.
References
Melzack R. The McGill Pain Questionnaire: major properties and scoring methods. Pain. 1975;1(3):277–299. https://pubmed.ncbi.nlm.nih.gov/1235985/
The foundational work behind using pain quality descriptors (sharp, burning, electrical, throbbing, etc.) as diagnostic information — not just a number. The idea that how pain feels carries clinical signal is well-established.Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2–15. https://pubmed.ncbi.nlm.nih.gov/20961685/
Explains why some pain systems become "wound up" over time — why irritability increases, why the threshold for pain drops, and why the 24-hour behavior of symptoms often tells you more than a single-point intensity rating.
Disclaimer
This article is educational and not medical advice. If you’re unsure about symptoms or have red flags, consult a qualified healthcare professional.