What's Actually Causing Your Sciatic Pain — And Why the Location Changes Everything
Sciatic pain is one of the most common complaints that brings people through our door. It's also one of the most frequently misunderstood.
Most people describe it the same way: a sharp, burning, or radiating sensation that runs down one side of the body — from the lower back or glute, through the back of the thigh, sometimes all the way to the foot. It can range from a dull ache to a sensation that stops you mid-step. For some, it comes and goes. For others, it's been a consistent presence for months or years.
Here's the part that often gets missed: sciatica is not a diagnosis. It's a symptom. If you've read our piece on why pain location rarely reveals the real problem, this idea will already be familiar — sciatica is one of the clearest examples of it.
The sciatic nerve is the longest nerve in the body. It runs from the lumbar and sacral spine, through the pelvis and deep hip muscles, and down each leg. When that nerve gets compressed or irritated — at any point along its path — you get the familiar radiating pain that people call sciatica.
Where the compression is happening determines everything. The exercises that help one person can aggravate another. The movement cues that reduce symptoms in a spinal case can be exactly wrong for a hip case. Understanding the origin is not an academic exercise — it's the difference between making progress and spinning your wheels.
This article breaks down the two most common origins of sciatic pain: the lumbar and sacral spine, and the hip (specifically, a condition called piriformis syndrome). We'll look at what drives each one, what the contributing factors look like in the body, and why getting this distinction right is the foundation of any sensible approach.
The Two Origins of Sciatic Pain
Before we go further, it helps to understand the nerve itself.
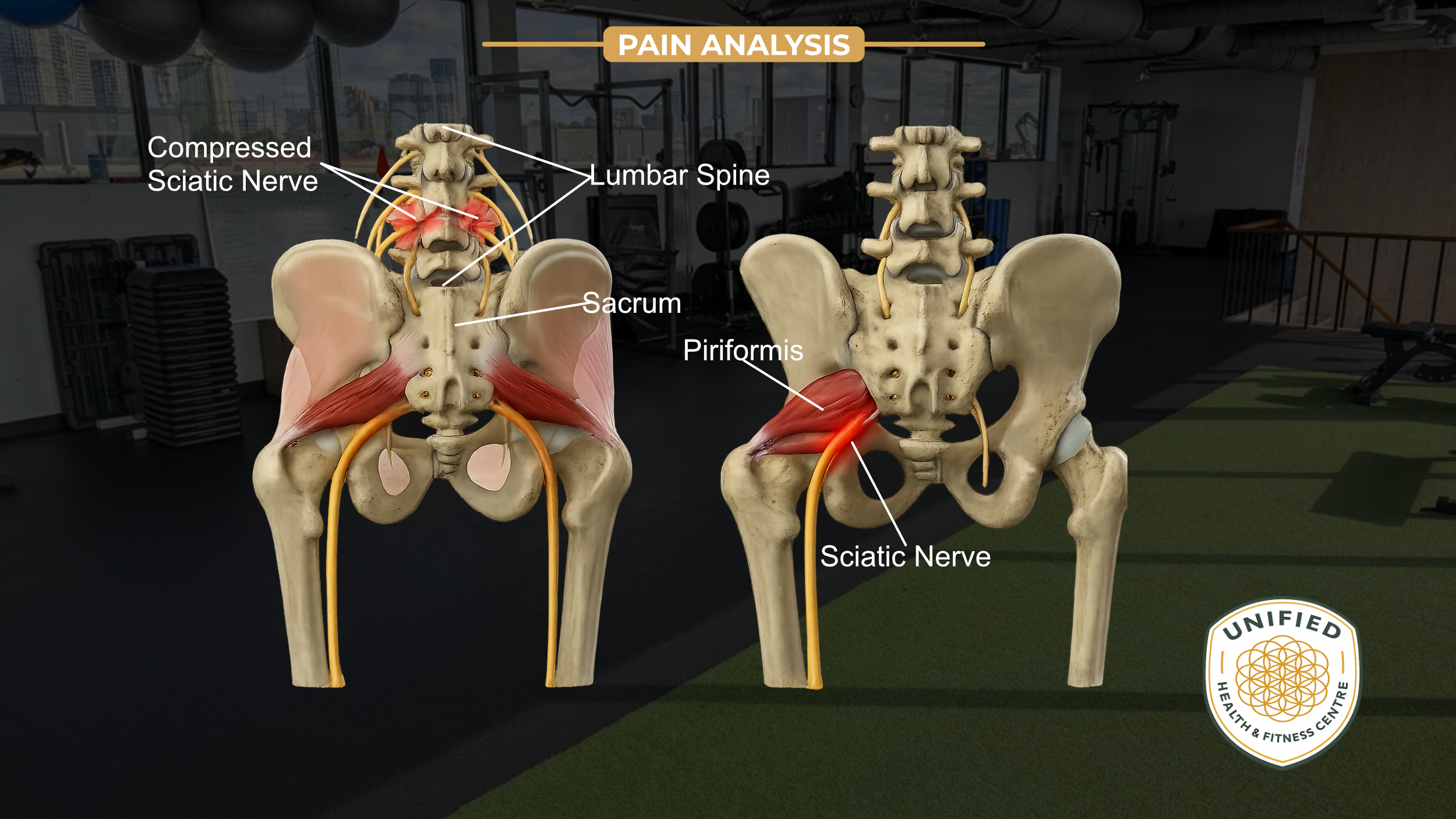
The sciatic nerve is formed from nerve roots that exit the lumbar spine at L4 and L5, and the sacrum at S1, S2, and S3. Those roots converge into a single nerve that travels through the pelvis, passes under (and sometimes through) the piriformis muscle in the hip, and continues down the back of the leg.
Compression can happen at two primary locations:
At the spine — where the nerve roots exit the lumbar or sacral vertebrae
At the hip — where the sciatic nerve passes through or adjacent to the piriformis muscle
Both produce similar pain patterns. But the mechanism, the contributing factors, and the appropriate response are meaningfully different.
Origin 1: The Lumbar and Sacral Spine
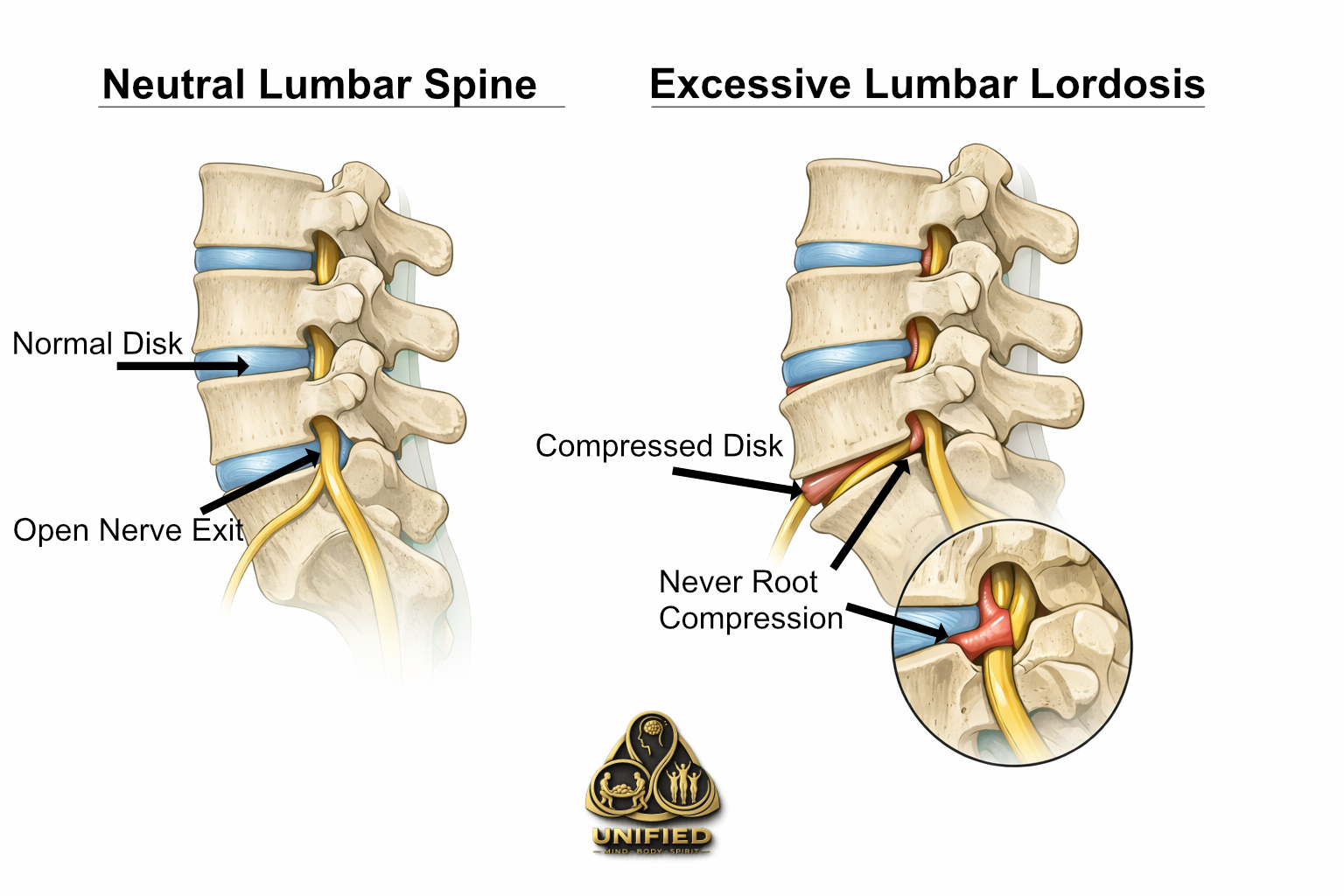
When sciatic pain originates at the spine, the nerve root is being compressed as it exits between the vertebrae. The most common structural driver of this is excessive lumbar lordosis — an exaggerated inward curve of the lower back.
Here's what happens mechanically: the lumbar spine has a natural curve, and that curve is functional. But when that curve becomes excessive — whether from posture habits, tight hip flexors, weak abdominals, or prolonged sitting — the posterior (back) surfaces of the lumbar vertebrae are driven closer together. The spaces through which the nerve roots exit, called the intervertebral foramina, narrow as a result.
In a normal lumbar curve, there's adequate space for the nerve. In an excessively curved lumbar spine, the posterior edges of adjacent vertebrae effectively begin to close in on those exit points. The nerve root gets compressed. You feel it as pain, tingling, or numbness radiating down the leg.
In more significant cases, this same mechanism can be a factor in disc pathology — where the contents of an intervertebral disc bulge posteriorly and press directly on a nerve root. But even without a disc issue, the simple mechanical loading from an excessive lumbar curve is enough to produce consistent nerve irritation.
What typically contributes to excessive lumbar lordosis:
Tight hip flexors — when the muscles at the front of the hip are shortened (common with prolonged sitting), they pull the pelvis into an anterior tilt, which increases the lumbar curve
Weak deep abdominals — the deep stabilizers of the spine help control lumbar position; when they are underactive, the lumbar spine defaults to compression
Tight lumbar extensors — muscles like the erector spinae, when overactive, hold the lumbar spine in extension
Underactive glutes — when the glutes are not generating force effectively, the lumbar extensors compensate, contributing to the same anterior pelvic tilt
The common thread is a pelvis that is being pulled forward and a lumbar spine that is being pushed into extension — narrowing the very spaces the nerve roots need.
For a deeper look at how this pattern plays out across a range of lower back presentations, see our article on why lower back pain keeps coming back.
Origin 2: The Hip — Piriformis Syndrome
Piriformis syndrome refers to compression of the sciatic nerve at the hip, caused by the piriformis muscle.
The piriformis is a small, deep muscle that runs from the front of the sacrum to the top of the femur (the greater trochanter). Its job is to externally rotate the hip. The sciatic nerve runs directly beneath it — and in approximately 17% of the population, passes directly through it.
When the piriformis becomes overactive, shortened, or dysfunctional, it can tighten around the sciatic nerve and produce the same radiating pain pattern as a spinal nerve root compression — even when the spine itself is fine.
This distinction matters clinically. Many people with piriformis-driven sciatica have been told they have a disc problem or a spinal issue, undergo imaging that shows something, and then follow protocols aimed at the spine — without improvement. That's because the nerve isn't being irritated at the spine. It's being irritated at the hip.
For a broader look at how the hip becomes a driver of referred pain and why generic hip treatments often fall short, see our article on hip pain that won't go away.
What typically drives piriformis overactivity:
The piriformis doesn't become a problem on its own. It becomes a problem when it's compensating for muscles that aren't doing their jobs. The following are the most common contributing factors:
Inactive Glutes
The glutes — particularly gluteus maximus — are the primary external rotators of the hip. When they are underactive, the piriformis takes on a disproportionate share of that external rotation demand. Over time, it becomes shortened and overloaded. A hyperactive piriformis in the presence of underactive glutes is one of the most common setups for hip-origin sciatica.
Leg Internal Rotation and Knee Valgus (Knee Knock)
When the femur consistently rotates inward — a pattern often visible as the knees tracking inward during walking, squatting, or standing — the piriformis is put under sustained stretch and demand. The body's attempt to control this rotation falls to the piriformis when the glutes aren't managing it. Knee valgus (knees caving inward, sometimes called "knock knees") is a visible downstream signal of this pattern.
Weak Lower Abdominals
The deep abdominal wall — particularly the transverse abdominis — plays a critical role in stabilizing the pelvis from below. When this system is weak, the pelvis loses its stable base. The hip musculature, including the piriformis, has to work harder to compensate for that pelvic instability. A pelvis that shifts or tilts under load creates a cascade of compensations in the surrounding musculature.
Weak Hamstrings
The hamstrings share the job of controlling the femur and pelvis with the glutes. When the hamstrings are underactive or lengthened (as they often are in people who sit for long periods), the hip loses an important stabilizing influence. This places more demand on the piriformis to maintain hip position.
Hyperactive or Shortened Quadriceps
Tight quadriceps — particularly the rectus femoris, which crosses the hip — pull the pelvis into an anterior tilt, similar to tight hip flexors. This affects the alignment of the entire hip complex and changes the mechanical environment the piriformis is working in. Shortened quads also limit hip extension, which forces compensatory patterns in both the lumbar spine and the hip rotators.

Why Distinguishing the Two Matters
Both types of sciatic pain can look identical from the outside. Both can cause radiating pain down the leg. Both can be aggravated by sitting, walking, or loading the hip and back.
But the management is different in important ways.
For spine-origin sciatica, the priority is reducing compression at the lumbar nerve roots. That often means addressing the anterior pelvic tilt, restoring length in the hip flexors and lumbar extensors, improving deep abdominal function, and gradually reloading the spine in positions that don't drive the lumbar into excessive extension.
For piriformis syndrome, the priority is reducing the demand on the piriformis itself. That means activating the glutes so they take back their role in hip control, addressing the internal rotation pattern, improving the stability of the pelvis through the lower abdominals and hamstrings, and restoring length in the shortened quads and hip flexors that are creating the mechanical environment for the problem.
In practice, there is often overlap — a person can have features of both. But the starting point still has to be an accurate read of what's driving the primary irritation. Loading glutes aggressively in someone whose sciatic pain is genuinely coming from a compressed nerve root, for example, can aggravate rather than help. Going straight to lumbar-focused stretching in someone with piriformis syndrome will produce limited results.
This is one of the core reasons that assessment precedes programming. Not as a formality, but because the intervention depends entirely on the finding.

What a Sensible Approach Looks Like
If you've been dealing with sciatic pain — whether it's been weeks or years — the most important thing you can do is resist the urge to start randomly treating it.
That sounds obvious, but the instinct for most people is to find a stretch, a YouTube video, or a protocol and start applying it. Some of those tools are fine in isolation. The problem is applying the wrong tool — and doing it repeatedly — because you haven't identified where the issue is actually coming from.
A proper assessment, in this context, involves looking at how the pelvis sits at rest, how the lumbar spine is loaded, whether there's evidence of anterior tilt, what the hip rotation pattern looks like, whether the glutes are generating force in basic movement patterns, and how the abdominals are functioning under load. From that picture, you can start to form a reasonable hypothesis about where the nerve is being irritated and what's driving it.
That's not a complicated process. But it does require looking before prescribing.
At Unified Health & Fitness in Etobicoke, our process starts with a complimentary initial consultation — a structured conversation that builds a clear picture of your history, your habits, and the patterns that are likely contributing to what you're experiencing. From there, a comprehensive movement and postural assessment identifies the mechanical factors driving the issue, and programming is built around that, not around a generic sciatica protocol.
If you've been dealing with sciatic pain and haven't found a clear answer, the starting point isn't another exercise. It's a clearer understanding of where the problem is actually coming from.
Book a complimentary consultation at Unified Health & Fitness →
We're located at 16 Newbridge Road #10, Etobicoke, ON M8Z 2L7. You can reach us by phone at 416-239-4550 or by text at 647-330-4205.
FAQ (for people trying to sort this out)
-
Most “sciatica” is just the sciatic nerve being irritated somewhere along its path.
The two most common buckets are:
Spine/nerve root irritation (lumbar or sacral) — the nerve gets compressed or sensitized as it exits the spine
Hip/piriformis irritation — the nerve gets irritated where it passes under (or sometimes through) the piriformis muscle
Other issues can mimic sciatica too (hamstring tendon irritation, SI joint referral, etc.). That’s why location alone isn’t enough.
-
You usually sort it by triggers + where it starts + what changes it.
If it’s more back-driven, symptoms often track with spinal positions (bending, extending, prolonged posture) and you may feel it start in the low back before it runs down.
If it’s more hip-driven, symptoms often feel like they start deep in the glute, and are more sensitive to hip rotation, walking patterns, single-leg loading, or sitting on the affected side.
It’s not perfect, and overlap is common — but those clues point you to the right “next thing to test.”
-
Yes.
If the piriformis is overactive/shortened (often because the glutes aren’t doing their job), it can compress or irritate the sciatic nerve at the hip and create the same radiating symptoms people associate with a “disc.”
-
Two common reasons:
Hip flexion + pelvic position: Sitting puts your hips flexed for long periods, which can change pelvic position and increase irritation — either at the spine (more compression) or at the hip (more pressure around the nerve).
Sustained pressure + low movement: You’re in one posture, often with pressure through the glute on one side, and the tissues don’t get a chance to “de-load.”
A helpful clue is what happens when you stand up and walk for 2–5 minutes — better, worse, or no change.
-
The honest answer: the right ones depend on the driver.
For spine/nerve root cases, the early win is usually reducing the positions that keep the low back compressed, restoring hip flexor length, and rebuilding abdominal control so the lumbar spine isn’t living in extension.
For piriformis cases, the early win is usually restoring glute contribution and cleaning up the internal-rotation/knee-valgus pattern so the piriformis isn’t doing all the work.
If an exercise gives you a short-term “stretch relief” but your symptoms keep returning, that’s usually a sign you’re treating sensation, not the mechanism.
-
If it’s not clearly improving within a couple weeks, if it keeps recurring, or if you’re stuck guessing and cycling through random stretches — it’s worth getting assessed.
And if you have progressive weakness, numbness that’s rapidly worsening, or any bowel/bladder changes, that’s a medical red flag and you should seek urgent medical evaluation.
References
Deyo RA, Weinstein JN. Low back pain.N Engl J Med. 2001;344(5):363-370.
Smoll NR. Variations of the piriformis and sciatic nerve with clinical consequence: a meta-analysis.Clin Anat. 2010;23(1):8-17.
Boyajian-O'Neill LA, McLain RL, Coleman MK, Thomas PP. Diagnosis and management of piriformis syndrome: an osteopathic approach.J Am Osteopath Assoc. 2008;108(11):657-664.
Neumann DA. Kinesiology of the hip: a focus on muscular actions.J Orthop Sports Phys Ther. 2010;40(2):82-94.
Unified Health & Fitness Centre — Private personal training in Etobicoke, Toronto. Serving Etobicoke, Mimico, Long Branch, Islington, and surrounding areas.